“I am approaching end-stage renal disease (ESRD). Can I do dialysis at home?”
Being diagnosed with kidney failure is a lifealtering event. The change can be very difficult, and many people find themselves with feelings of anxiety and stress while waiting for a transplant. The diagnosis can be particularly stressful because it not only involves changes in your physical health, but in your work, family life and relationships.
As a first measure, your doctor will most likely suggest a change in diet. By carefully managing your diet you can minimize the accumulation of waste products and extra fluids in your blood, and thus help your kidneys. Paying attention to what you drink can do some of the work that healthy kidneys do in maintaining the right fluid balance in your body.
Depending on the stage of kidney failure, most likely a change in diet alone will not be enough to treat your disease. Patients approaching ESRD must choose a dialysis option for treatment.
Deciding what dialysis treatment is right for you can be overwhelming. But the more you know, the better you’ll be able to make the best choice for your life. “Knowing your options is empowering,”explains Miguel Torres, a patient currently on home dialysis. Miguel currently educates and trains patients in Chula Vista, Calif. He believes understanding your treatment options gives you greater control over your life. “My treatment choice has enabled me to continue my lifestyle and allowed me to do more than I thought I’d be able to do. There’s freedom in knowing your options.”For his treatment, Miguel chose peritoneal dialysis (PD), one of several at-home dialysis options.
Your At-Home Options
Peritoneal Dialysis (PD) is a home dialysis treatment used around the world today. PD works inside the body, using the peritoneal membrane, or abdominal lining, as a natural filter to remove excess fluid and waste from the body. No needles are required, and blood never leaves the body. Dialysis fluid is placed in the peritoneal cavity through a tube, called a PD catheter, surgically inserted in the abdomen. Excess fluid and waste travel from the blood across the peritoneal membrane into the dialysis fluid, which is then drained from the abdomen.
Two Types of PD:
Continuous Ambulatory Peritoneal Dialysis (CAPD): Patients manually infuse fresh PD solution and drain the used solution (also known as an “exchange”). On average, a solution exchange takes 30-45 minutes to perform, and solution exchanges occur three to five times each day.
Automated Peritoneal Dialysis (APD): Patients hook up to a machine that automatically performs solution exchanges, usually overnight while the patient sleeps each night, lasting anywhere from six to eight hours.
Most patients are medically eligible for PD. Studies have shown that PD patients have high levels of satisfaction with their therapy and high levels of personal well-being. PD can offer more time for family and social activities and is a good choice for patients who are employed.
Home Hemodialysis (HHD) is an additional home-based treatment option for people living with end-stage renal disease (ESRD). During hemodialysis (HD), blood is pumped from the body through a machine containing a filter, called a dialyzer, which cleans the blood and returns it to the body. HHD is a form of HD using a machine modified for use in the home. It can be done at night while the patient is asleep, or during the day. It typically is done three to six times a week. The length of the dialysis sessions varies. If done during the night while the patient sleeps (nocturnal HD), it usually lasts anywhere from six to eight hours. If done during the day (short daily HD), the treatments are usually from two to four hours.
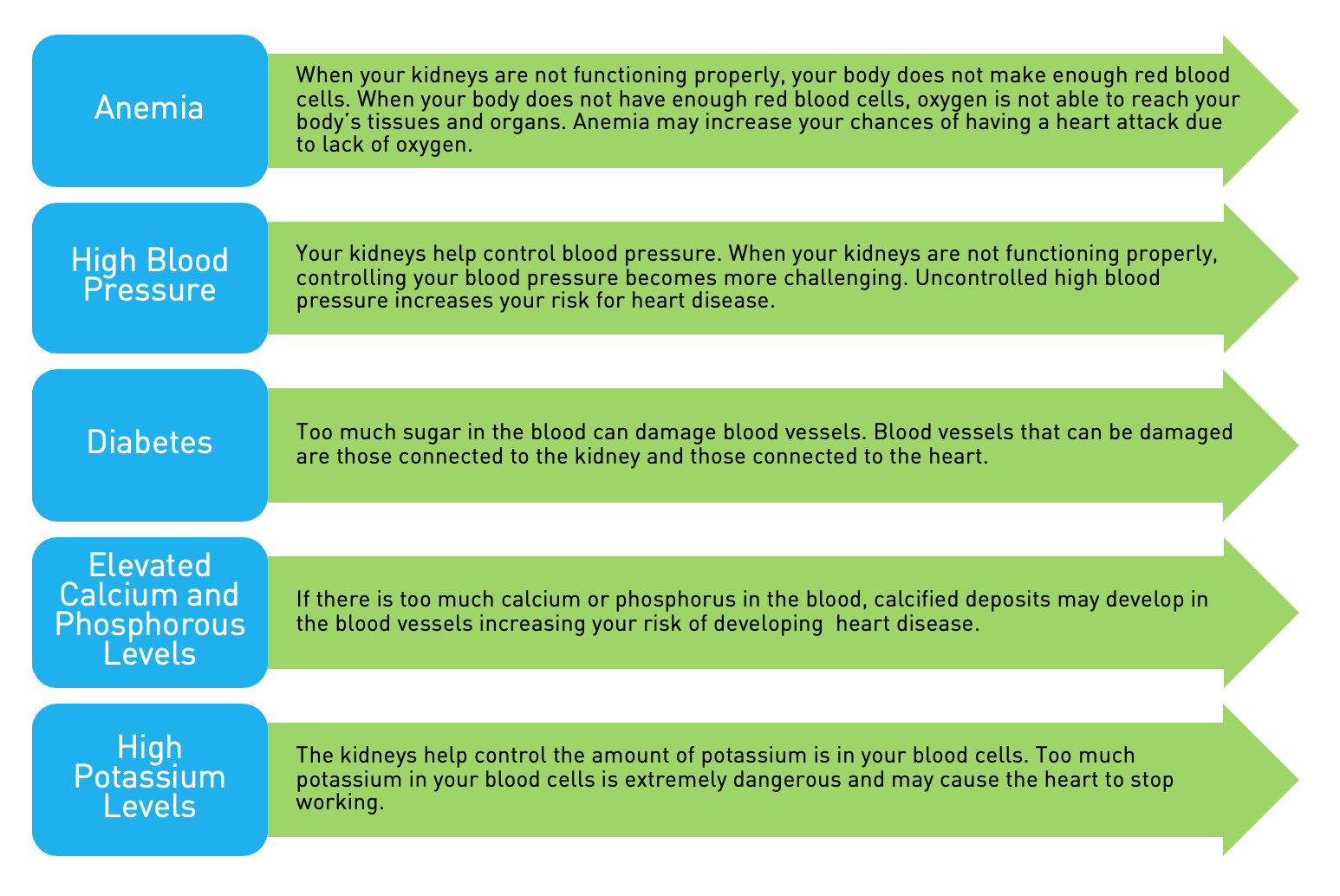
When people living with end-stage kidney disease are able to have their treatment at home, physicians and patients are afforded more flexibility in prescribing a treatment schedule that is best for the patient. Observational studies suggest newer approaches to home dialysis treatments can offer key clinical advantages such as improvements in blood pressure, phosphate levels, and measures of cardiac function, as well as reduced sleep apnea (temporary breathing interruption during sleep), and the ability to carry a baby full-term in women. In addition to the clinical benefits of daily dialysis, patients experience significantly better lifestyle advantages, particularly if patients can dialyze for longer periods of time, such as at night.
Home dialysis may not be appropriate for everyone, and your doctor can help you decide if you are eligible for a home dialysis therapy. For example, patients must be willing to perform the therapy themselves or with the assistance of a caregiver. Since it is done at home, appropriate space for supplies must be available. As with any treatment, care must be taken by always using proper sanitary technique and catheter care. It is important to talk with your doctor to understand these and other risks that exist with any type of dialysis therapy.
Ultimately the choice is up to you and your doctor. Being a well-educated and knowledgeable patient will help you make an empowered decision. While waiting for a transplant, the appropriate treatment and management in the early stages of kidney failure may slow the progression of the disease. In addition to exploring treatments with your physician, it may be a good idea to share your options with your friends and family. With their support and guidance from your doctor, you’ll be able to choose the treatment that best suits your condition and lifestyle.
Bruce Culleton, MD, completed his Internal Medicine and Nephrology Training in Canada in 1999. He is currently Senior Medical Director for Baxter Healthcare in Illinois and Adjunct Associate Professor at the University of Calgary, Alberta, Canada. During his seven years in Calgary he served as Medical Director for the Peritoneal Dialysis and the Progressive Kidney Disease Programs. His publications include many related to CKD epidemiology and clinical trials in dialysis.
This article originally appeared in the November 2009 issue of At Home with AAKP.